Exploring the Delayed Cardiac Effects of Electrical Burns: A Case Report on Myocardial Infarction
Aug 23, 2024
2024/8/22
This case report titled ‘A Case Report: Revealing Delayed Cardiac Phenomenon in Electrical Injuries‘ examines a rare situation where a patient experienced delayed cardiac issues days after sustaining an electrical burn injury.
Electrical burns, although rare, can have significant consequences, particularly on the heart. The study focused on a 28-year-old tile builder who sustained high-voltage electrical shock, resulting in burns and unconsciousness. His electrocardiograms (ECGs) appeared normal at first, but by the third day, cardiac changes appeared, signaling myocardial infarction.
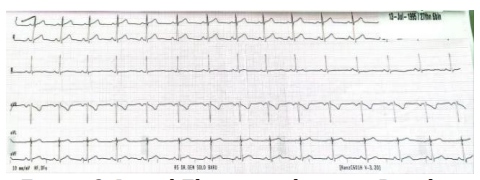
1. The patient initially presented with superficial and deep dermal burns, covering 36% of his body, and his vital signs were stable. Early ECGs showed no abnormalities, but doctors monitored him for potential delayed effects.
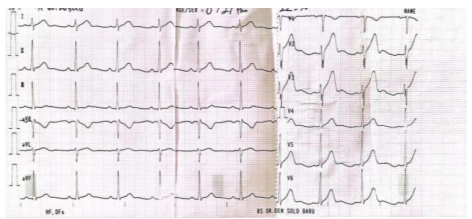
2. On the third day, ECGs showed ST-segment elevation and hyperacute T waves, indicative of myocardial infarction. At this point, his Troponin I levels had risen significantly to 4.81 ng/mL.
3. The case emphasizes the importance of interdisciplinary care involving burn surgeons, cardiologists, and neurologists. Continuous monitoring is essential for identifying and managing complications that develop after electrical injuries.
4. Treatments included heparin infusion, along with isosorbide dinitrate and clopidogrel. The patient’s condition improved after treatment, but it underscores the need for early and continuous intervention.
Electrical burns are rare but serious injuries that can lead to significant long-term complications, particularly affecting the heart. This case report examines a rare scenario in which a 28-year-old male experienced cardiac complications days after sustaining an electrical burn, underscoring the importance of continuous monitoring and a multidisciplinary approach in such cases.
Method
The study describes the case of a patient who sustained electrical burns and outlines the monitoring methods employed, including daily electrocardiograms (ECGs) and troponin level assessments. The case was managed using standard burn treatment protocols, along with specific cardiac care interventions like heparin infusion and medications such as isosorbide dinitrate and clopidogrel.
Result
1. Initial Presentation and Findings
The patient initially presented with burns over 36% of his body, a significant portion of which affected both superficial and deep dermal layers. On admission, his vital signs were stable, and initial diagnostic tests, including an electrocardiogram (ECG), did not reveal any significant abnormalities. His vital signs included a heart rate of 71 beats per minute, blood pressure of 133/85 mmHg, and normal respiratory function, all within expected parameters.
Given the patient’s history of exposure to high-voltage electricity, a Glasgow Coma Scale score of 15 indicated full consciousness, with no immediate neurological deficits. Despite the absence of immediate cardiac symptoms, it was clear that further monitoring was crucial due to the well-documented risks of delayed cardiac events following electrical burns.
Following standard burn injury protocols, the medical team initiated intravenous fluid resuscitation to stabilize the patient’s condition. The early signs of cardiac stability, however, did not eliminate the risk of potential complications. As a result, continuous monitoring of cardiac enzymes and daily ECGs were performed to detect any developing abnormalities.
Initial findings showed no immediate cardiac abnormalities, but continuous monitoring was crucial given the high risk of delayed complications.
2. Development of Myocardial Infarction
On the third day of hospitalization, significant changes in the patient’s cardiac condition were observed. Daily ECG monitoring revealed ST-segment elevation in leads II, III, and avF, and hyperacute T waves in leads V2 to V4. These findings were indicative of an evolving myocardial infarction (MI), most likely triggered by the earlier electrical injury. The cardiac event was further supported by an increase in serum troponin I levels, which rose dramatically to 4.81 ng/mL on the same day, confirming the myocardial damage.
Troponin I is a highly specific biomarker for myocardial injury, and its marked increase provided strong evidence that the electrical shock had caused delayed damage to the heart muscle. While the initial ECG had been normal, the latent effects of the injury began to manifest, underscoring the delayed nature of cardiac complications in electrical burns.
In addition to the troponin I elevation, the patient exhibited signs of cardiac ischemia, although he remained clinically stable. His blood pressure remained within the normal range, and no significant symptoms such as chest pain were reported. However, the ECG changes were highly suggestive of underlying ischemic damage that could have led to more serious complications if left untreated.
The development of myocardial infarction three days post-injury highlights the delayed onset of electrical burn-induced cardiac complications.
3. Cardiac Management and Outcome
Upon detecting the myocardial infarction, the medical team initiated a comprehensive treatment plan aimed at stabilizing the patient’s cardiac condition. A heparin infusion was started at a rate of 12 units/kg/hour to prevent further clot formation, along with antiplatelet therapy using 75 mg of clopidogrel and 5 mg of isosorbide dinitrate. The latter medication was crucial in controlling the vasospasm that may have contributed to the ischemic event.
In addition to the pharmaceutical interventions, the patient was placed under continuous cardiac monitoring to track further changes in his ECG and troponin levels. Over the next few days, the patient’s condition stabilized, with a gradual decrease in troponin I levels and improvement in the ST-segment elevation observed in subsequent ECGs.
Despite the delayed onset of the myocardial infarction, early detection and aggressive treatment helped prevent further deterioration of the patient’s cardiac function. The patient did not exhibit any further complications, and his cardiac biomarkers eventually returned to near-normal levels. However, this case underscores the importance of long-term cardiac follow-up for patients with electrical burns, even if they initially appear stable.
Timely intervention and aggressive management prevented the progression of myocardial injury and contributed to the patient’s recovery.
Conclusion
This case study highlights the hidden and delayed nature of cardiac complications in patients with electrical burns. The need for prolonged monitoring and interdisciplinary care is essential in preventing severe outcomes. Future research should focus on improving the early detection and management of such complications to enhance patient outcomes.