Advances in Cardiovascular Research: New Approach to Alleviate Cardiac Injury from Electric Shocks
Aug 22, 2024
2024/8/22
In a groundbreaking study, researchers explored the mechanisms behind electric shock-induced cardiac injury and evaluated the efficacy of a novel compound to reduce the extent of damage. This study focused on human cardiomyocytes, where exposure to electric shocks during cardiopulmonary resuscitation (CPR) can cause significant cellular damage. The research is notable for its implications in reducing post-cardiac arrest mortality rates.
1. Researchers used two types of electric fields: nanosecond pulsed electric field (nsPEF) and microsecond pulsed electric field (µsPEF) to evaluate their effects on cell damage and death.
2. The application of Poloxamer 188 (P188) was found to be significantly effective in reducing cellular death, particularly when applied immediately after exposure to electric pulses.
3. The study identified differences in cell death mechanisms triggered by nsPEF and µsPEF, with nsPEF inducing necrosis and µsPEF triggering apoptosis.
4. The use of P188 showed promise in promoting membrane repair and reducing both necrosis and apoptosis in treated cardiomyocytes, offering potential for post-CPR recovery enhancement.
Cited from: How to alleviate cardiac injury from electric shocks at the cellular level
Author: Pamela W. Sowa, Aleksander S. Kiełbik, Andrei G. Pakhomov, Emily Gudvangen, Uma Mangalanathan, Volker Adams, Olga N. Pakhomova
DOI: http://doi.org/10.3389/fcvm.2022.1004024
Introduction
Electric shocks are the only effective therapy for ventricular fibrillation, but they can cause cardiac injury, contributing to post-cardiac arrest syndrome. The study explores the use of Poloxamer 188 (P188) in preserving membrane integrity and reducing cell death in human cardiomyocytes exposed to electric shocks during CPR. Researchers aim to alleviate the myocardial damage caused by these electric shocks.
Method
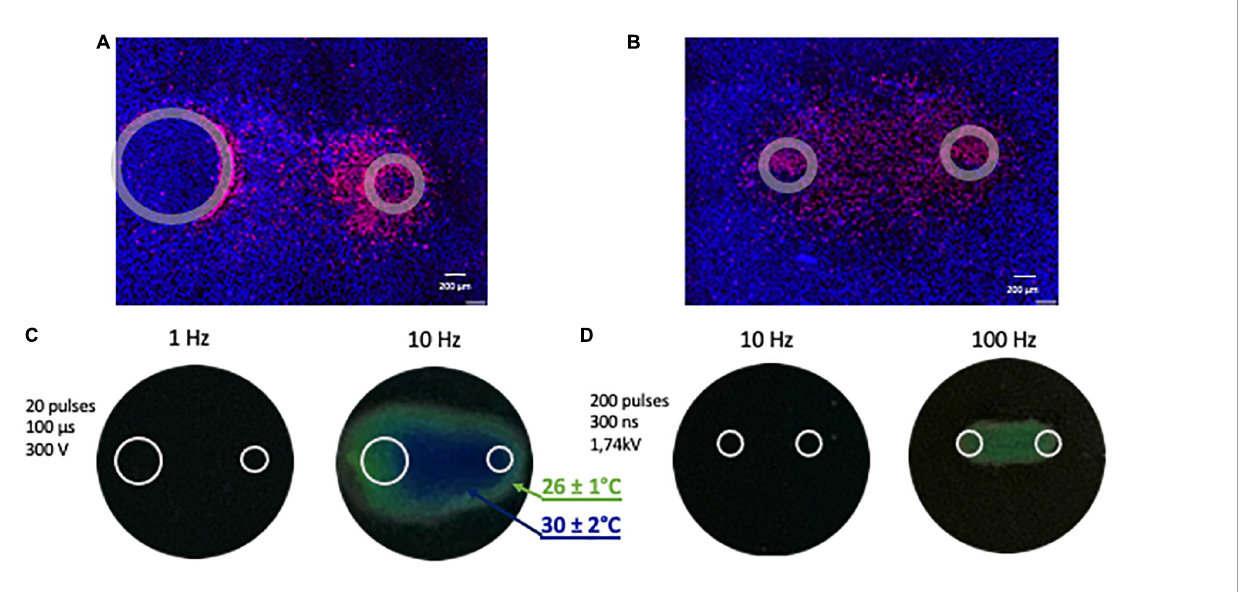
In this research, human cardiomyocytes were exposed to nanosecond (nsPEF) and microsecond pulsed electric fields (µsPEF) to study their effects on cell death. The study used a custom-built 3D printer with electrodes positioned orthogonally to the cell monolayers. P188 was added after the electric shocks to assess its ability to mitigate damage. The cell death and viability were measured at different time points using fluorescent microscopy, and electric field simulations were performed to determine field strengths across samples.
Result
1. Poloxamer 188 Reduces Cell Death After nsPEF Shocks
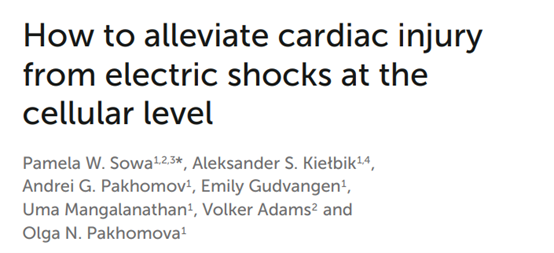
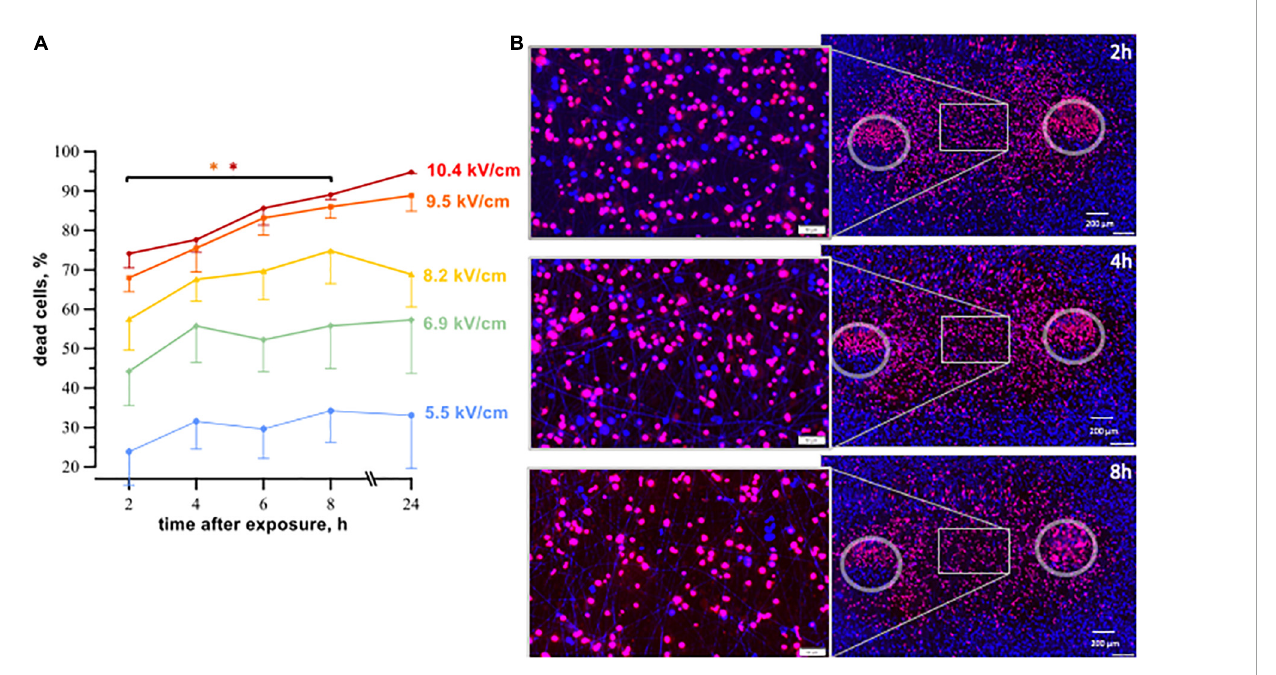
The results showed that Poloxamer 188 (P188) was highly effective in reducing cardiomyocyte death after exposure to nsPEF shocks. Initially, when cardiomyocytes were subjected to 200 pulses of 300-ns duration at a strength of 1.74 kV/cm, the cell death reached as high as 97% within 8 hours. When different concentrations of P188 were applied 10 seconds after the electric shock, the mortality rate of the cardiomyocytes dropped dramatically.
At the highest concentration of P188 (1%), cell death was reduced to 58%, marking a significant decrease compared to the untreated group. Lower concentrations of 0.5% and 0.2% also showed reductions in cell death, with mortality rates falling to 68% and 75%, respectively. These reductions in cell death suggest that P188 has a strong protective effect against the damage caused by nsPEF shocks, particularly at higher concentrations, effectively reducing the percentage of necrotic cells.
The protective effect of P188 became more pronounced as the strength of the electric field increased. Cells exposed to higher field strengths showed greater susceptibility to cell death without treatment, but P188 mitigated this damage, even in stronger electric fields. These findings indicate that P188 is particularly effective in reducing necrotic cell death caused by nsPEF shocks, offering a potential therapeutic intervention to reduce damage from defibrillation-induced injury.
2. Poloxamer 188 Mitigates Apoptosis After µsPEF Shocks
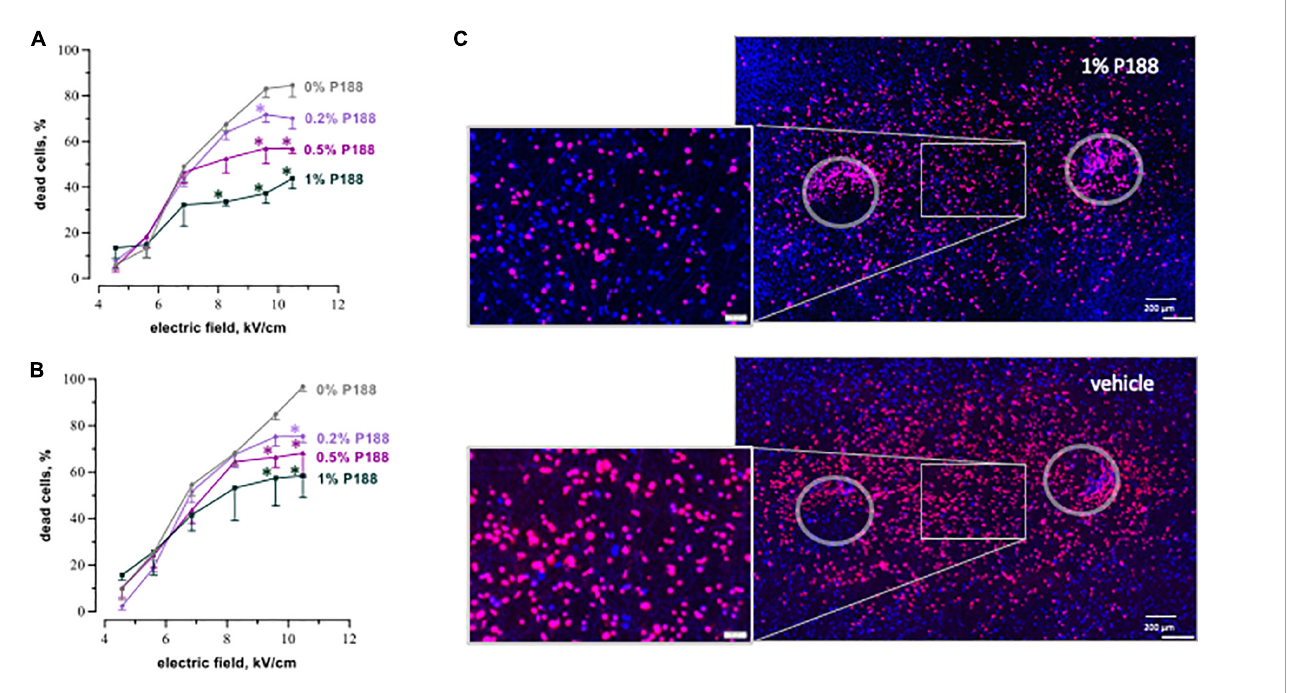
In addition to reducing necrosis caused by nsPEF shocks, P188 also mitigated apoptotic cell death induced by µsPEF shocks. The µsPEF shocks caused apoptosis in cardiomyocytes, with caspase 3/7 activity peaking at 2 and 4 hours after exposure to 20 pulses of 100-µs duration at 300 V. The increase in caspase 3/7 activity was a clear indicator of programmed cell death.
When P188 was applied at concentrations of 0.5% and 0.2%, the percentage of apoptotic cells decreased significantly, as shown by the reduction in caspase activity over 24 hours. At 0.5% concentration, the number of dead cells was reduced by nearly 50%, showing a sharp contrast between treated and untreated groups. While P188 at 1% did not show the same level of effectiveness, likely due to potential cytotoxicity, the lower concentrations of P188 proved highly effective in reducing apoptosis.
By reducing both necrotic and apoptotic cell death, P188 demonstrates its versatility as a therapeutic agent capable of addressing multiple mechanisms of cell death. The results from these experiments suggest that P188 can be an important factor in preventing further cardiac injury after electric shocks during CPR, potentially improving patient outcomes.
3. Differentiated Time Course of Cell Death Between nsPEF and µsPEF
The study also revealed distinct differences in the timing of cell death between nsPEF and µsPEF shocks. Cells exposed to nsPEF shocks showed a rapid increase in cell death, with mortality reaching a maximum within 8 hours after exposure. In contrast, µsPEF shocks resulted in a more gradual increase in cell death, with the peak occurring between 16 and 24 hours post-exposure. This suggests that the mechanisms driving cell death differ between the two types of electric fields.
For nsPEF shocks, most of the cell death occurred through necrosis, as evidenced by the rapid uptake of propidium iodide (PI) dye within the first few hours. In contrast, µsPEF shocks led to the activation of apoptotic pathways, as indicated by the increase in caspase 3/7 activity. These differences in timing and cell death mechanisms are crucial for understanding how electric shocks affect cardiac cells and highlight the need for targeted therapeutic interventions, such as P188, which can address both necrosis and apoptosis.
Furthermore, the timing of P188 application played a critical role in its efficacy. The protective effect of P188 was most effective when administered within 10 seconds of the electric shock, suggesting that early intervention is key to preventing extensive cell death. This highlights the importance of timely therapeutic strategies in clinical settings, particularly during CPR and defibrillation procedures.
Conclusion
This study highlights the potential of Poloxamer 188 as a therapeutic intervention to reduce electric shock-induced cardiac injury by targeting both necrosis and apoptosis pathways. Future research could focus on testing P188 in clinical settings, offering promising avenues for improving outcomes after cardiac defibrillation.